Caesarian Section
What are the indications for caesarean sections. Explain the pre and post operative nursing care of mother with caesarean sections .
Definition
Delivery of the foetus through an incision on the abdominal wall and uterine wall
Indications
Contracted pelvis
Cephalopelvic disproportion
Uterine inertia
Placenta previa
Premature separation of placenta
Malposition
Malpresentation
Pre-eclampsia
Diabetes mellitus with big baby
Cardiac diseases
Vaginal scarring
Carcinoma or other tumours of the cervix preventing normal delivery
Cervical dystocia
A previous uterine incision with weak or tender scar
Prolapse of the umbilical prolapse
Foetal distress
Bad obstetric history (habitual IUD)
Failure of progress despite adequate stimulation
Contraindications
Death of foetus
Gross congenital malformations
Extreme prematurity
Coagulation defects
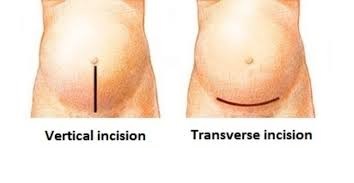
Types of Caesarian Section
Classical : Midline longitudinal/vertical incision on the abdomen and uterus - easy access and delivery of the baby, more prone to complications
LSCS (Lower Segment Caesarian Section) : Transverse incision on the abdominal wall and uterus. Lesser blood loss and easy to repair. Less prone for incisional hernias, infection, uterine rupture later is less
Timing of Caesarian Section
Elective
When done as a planned procedure : ensure optimal preoperative preparation
Emergency
When done because of sudden deterioration in maternal/fetal conditions or during labour due to non progress/failed induction/failed trial
Indications for Classical Caesarian Section
Possiblity of adhesions in the lower segment
Need for rapid delivery
Anterior placenta previa
Large fibroids in the lower uterine segment
Pregnancy with carcinoma with carcinoma cervix
Section done when the mother dies
Transverse lie
If the Caesarian section has to be followed by hysterectomy
Preoperative Preparations
Valid informed consent
Inj.Ranitidine 50mg IV half an hour before OT
Inj. Metoclopramide IV half an hour before OT
Stomach sholuld be empt
Bladder catherized
Check the fetal presentation, position and FHS recorded
Complications of Caesarian Section
Anesthetic complications
Respiratory Complications : due to pain & immobilization
Damage to ilioinguinal and iliohypogastric nerves and pain
Wound infection, hematoma, excessive edema
Deep Vein Thrombosis due to hypercoagulability, decreased venous tone
Injuries to intestines
Hemorrhage
Late complications : incisional hernia, scar rupture
Role of Physiotherapy
Teach how to mobilize early with least pain : demonstration
Teach how to cough with abdominal support
Deep breathing exercises
Exercises to improve blood circulation to prevent DVT
Post-operative Care
In recovery area : should be observed on a one-to-one basis until they have regained airway control and cardiorespiratory stability and are able to communicate.
Monitor level of consciousness, BP, Heart rate, respiration, vaginal bleeding
Women must be kept under clinical observation at all times and all measurements must be recorded
Automatic recording systems is encouraged.
The frequency of recordings will depend on the stage of recovery and clinical condition of the patient.
Non-invasive blood pressure, heart rate and rhythm, respiratory rate and continuous pulse oximetry every 5 minutes for the first 30 minutes in recovery
Pain intensity e.g. verbal rating scale
Early breast feeding started
Nil orally for 24 hours
Crystalloids IV fluids for 24 hours
Antibiotics as per hospital policy
Pain relief - opioids (pethidine, tramadol), NSAIDs per oral or patenteral, rectal (suppository) can be combined with opioid injections
Monitor vital parameters, vaginal bleeding, urine output, hydration
Palpate the uterine fundus and find the location, consistency
Encourage early breast feeding - stimulates contraction of the uterus
Women who are recovering well after CS and who do not have complications can eat and drink when they feel hungry or thirsty.Oral fluids after 24 hours
Removal of the urinary bladder catheter should be carried out once a woman is mobile after a regional anaesthetic and not sooner than 12 hours after the last epidural 'top up' dose.
Discharge after 4 days
Suture removal 7-10th day
Contraceptive advice
* * * * * * * * * * * * * *